RSNA Press Release
- Imaging findings in the lungs of H7N9 influenza patients include ground-glass opacity, consolidations, air bronchograms and interlobular septal thickening.
- H7N9 is a recently discovered subtype of avian influenza virus or “bird flu.”
- H7N9 can cause acute respiratory distress syndrome, organ failure and death.
New Study Describes Imaging Findings in H7N9 Influenza
Released: July 2, 2013
| Media Contacts: | |
| RSNA Media Relations: | 1-630-590-7762 |
| Linda Brooks 1-630-590-7738 lbrooks@rsna.org |
Maureen Morley 1-630-590-7754 mmorley@rsna.org |
OAK BROOK, Ill. — H7N9 pneumonia is characterized by imaging findings that differentiate it from other types of pneumonia, including rapidly progressive changes in the lungs and pulmonary connective tissues, according to the first study to describe radiologic findings in the disease. The results are published online in the journal Radiology.
"The severity of these findings is associated with the severity of the clinical condition of the patients," said study co-author Zhiyong Zhang, M.D., Ph.D., from the Department of Radiology at Shanghai Public Health Clinical Center and Shanghai Medical College of Fudan University in China.

H7N9 is a recently discovered subtype of avian influenza virus or "bird flu," Cases of bird flu infection in humans typically result from direct or close contact with infected poultry, such as domesticated chickens, pigeons or ducks, or with surfaces contaminated with secretions and excretions from infected birds. The first human outbreak of H7N9 was reported in China in March 2013. This new strain in humans has caused severe and rapidly progressing respiratory illness. H7N9 can cause acute respiratory distress syndrome, organ failure and death.
For the study, Dr. Zhang and colleagues evaluated the clinical data and radiologic files of 12 patients with avian-origin influenza A H7N9 virus who were admitted to Shanghai Public Health Clinical Center between April 3, 2013, and April 20, 2013. The 12 patients included nine men and three women, 47 to 81 years old (mean age, 66 years).
None of the patients raised pigeons or lived in or near a pigeon-infested area. One patient kept chickens at home, and four patients had gone to various farmers' markets before the symptom onset. All other patients had no clear history of exposure to poultry. All patients exhibited fever with temperature of 38°C to 40°C (100.4°F to 104°F), cough, shortness of breath, and white phlegm and loss of strength at the onset of the disease or within one week. They rapidly progressed to severe pneumonia and acute respiratory distress syndrome.
The intervals between the onset of symptoms and the initial imaging examinations ranged from one to six days for chest X-rays and two to nine days for computed tomography (CT).
Chest X-rays were taken every one or two days thereafter to monitor disease progression and treatment response. To evaluate disease progression and possible complications, 10 of the patients underwent follow-up CT two to eight days after initial examination.
The imaging findings included ground-glass opacity (a hazy area in the lungs with the appearance of ground glass) in all 12 patients, consolidations (regions of lung tissue filled with liquid) in 11 patients, air bronchograms (air-filled bronchi made visible by swelling in adjacent tissues) in 11 patients, and interlobular septal thickening (thickening of pulmonary connective tissue) in 11 patients. Lung lesions involved three or more lobes in all cases, but were mostly detected in right lower lobe. Follow-up computed tomography (CT) in 10 patients showed interval improvement of the lesions in three patients and worsening of the lesions in seven patients. Imaging findings closely mirrored the overall clinical severity of the disease.
"The distribution and very rapid progression of consolidations, ground-glass opacity, and air bronchograms, with interstitial changes, in H7N9 pneumonia help differentiate it from other causes of pneumonia," Dr. Zhang said.
While these imaging characteristics are similar to those found in other respiratory diseases, such as H1N1, H5N1 and severe acute respiratory syndrome (SARS), there are differences.
"Both H1N1 pneumonia and SARS distribute more peripherally, with more changes in the spaces between tissues, and progress less rapidly than H7N9," Dr. Zhang said. "In our study, the right lower lung was most likely to be involved, while there's no lobar predilection in findings of H5N1 influenza."
# # #
"Emerging H7N9 Influenza A (Novel Reassortant Avian-Origin) Pneumonia." Collaborating with Dr. Zhang were Qingle Wang, M.D., Yuxin Shi, M.D., Ph.D., and Yebin Jiang, M.D., Ph.D.
Radiology is edited by Herbert Y. Kressel, M.D., Harvard Medical School, Boston, Mass., and owned and published by the Radiological Society of North America, Inc. (http://radiology.rsna.org/)
RSNA is an association of more than 51,000 radiologists, radiation oncologists, medical physicists and related scientists, promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Ill. (RSNA.org)
For patient-friendly information on Chest X-ray and Chest CT, visit RadiologyInfo.org.
Images
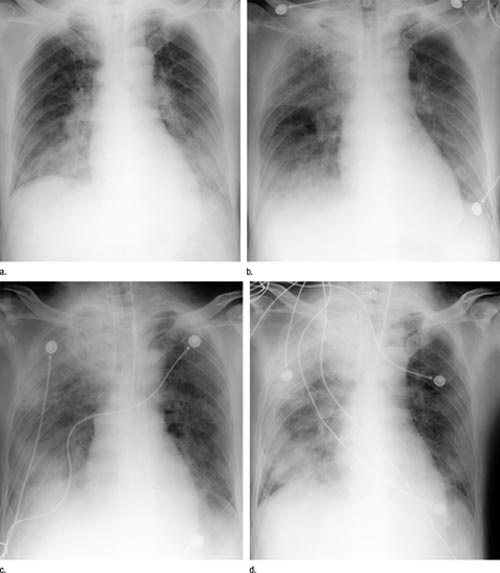 Figure 1 (a–d) Anteroposterior chest radiographs obtained with portable bedside unit in 56-year-old man with H7N9 influenza on (a) day 7, (b) day 8, (c) day 9, and (d) day 10 after onset of illness. The series of radiographs shows rapid daily progression of areas of increased opacity and consolida¬tion. A clear interlobar fissure margin is seen on day 8 (in b). (c) At 9 days after onset (3 days after admission), the patient’s condition deteriorated, with shortness of breath, chest distress, and blood oxygen saturation of 80%–85%, and the patient was intubated with an invasive ventilator. High-res (TIF) version (Right-click and Save As) |
 Figure 2 Axial thin-section CT image (section thickness, 1 mm) in 67-year-old man with H7N9 influenza shows extensive GGOs and consolidation and sporadic centrilobular nodules (arrows), which could hardly be appreciated at conventional CT. High-res (TIF) version (Right-click and Save As) |
 Figure 3 Axial thin-section CT image in 75-year-old woman with H7N9 influenza shows extensive GGOs and consolidation appearing as a geographic pattern and predominantly distributed in the right lung. Reticulation super¬imposed on GGOs (arrowheads), a centrilobular nodule (arrow), and a small amount of pleural effusion are also seen. High-res (TIF) version (Right-click and Save As) |
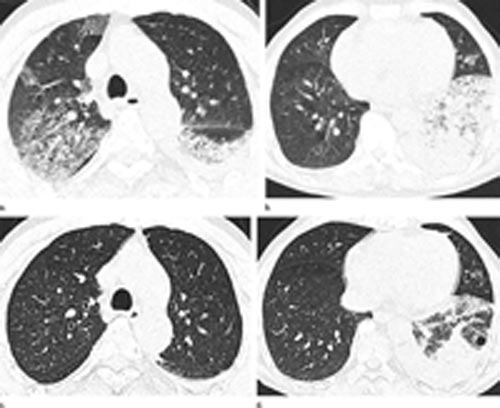 Figure 4 (a–d) Axial thin-section CT images in 65-year-old man with H7N9 influenza. (a, b) On initial images obtained at admission, extensive GGOs and consol¬idation can be appreciated. (c, d) Images obtained at 7-day follow-up show complete resorption of the lesion in the right upper lobe and partial resorption in the left lower lobe with a round cystic change. High-res (TIF) version (Right-click and Save As) |
 PDF
PDF{kind=link}