RSNA Press Release
- Using CT-fluoroscopy guidance, physicians are able to effectively treat most patients with palmar hyperhidrosis (sweaty hands) with a single 20-minute procedure.
- Percutaneous sympathectomy is less costly than surgery with fewer risks and complications.
- Up to three in every 100 Americans suffers from sweaty hands.
'No Sweat' CT-Guided Injection Treats Embarrassing Hand Condition
Released: November 29, 2005
| Media Contacts: | |
| RSNA Media Relations: | (630) 590-7762 |
| Maureen Morley (630) 590-7754 mmorley@rsna.org |
Heather Babiar (630) 590-7738 hbabiar@rsna.org |
CHICAGO - A minimally invasive procedure can permanently cure people who suffer from "sweaty hands," according to a study presented today at the annual meeting of the Radiological Society of North America (RSNA).
Computed tomography (CT) fluoroscopy allows precise needle guidance in the treatment of palmar hyperhidrosis, or sweaty hands, minimizing risk and discomfort to the patient.
"This CT-guided percutaneous technique is the most secure treatment today and stops sweating from the hands to the armpits with very little chance of recurrence," said the study's lead author, Hugues Brat, M.D., head of the radiology department at Centre Hospitalier Hornu - Frameries, in Hornu, Belgium.
Up to three out of every 100 people in the United States faces social and professional discomfort due to sweaty hands. The condition is caused by an overactivity of the sympathetic nervous system. Previously, the only known permanent treatments for sweaty hands were thoracic conventional or endoscopic surgical sympathectomies requiring general or local anesthesia. Both procedures are secure but can produce serious complications, ranging from bleeding and collapsed lung to partial paralysis and Horner syndrome, which affects movement of the eyelid.
Minimally invasive treatments are available which effectively treat sweaty hands with varying degrees of effectiveness, cost and risk to the patient. Some physicians offer local Botox injections, which are efficient but are painful and expensive and only last six months.
Percutaneous sympathectomy with CT fluoroscopy is a 20-minute procedure requiring no anesthesia, with no risk of nerve damage or bleeding and only minimal risk of Horner syndrome. Most patients require a single treatment for each side. As with surgical sympathectomy, there is an unpredictable but rare risk of compensatory sweating at the level of the chest.
For the procedure, interventional radiologists make a single needle puncture through the upper back and, using CT guidance, inject a phenol-based medication that interrupts the nerve tracts and nodes that transmit signals to the sweat glands. "This is the most precise and effective treatment of palmar hyperhidrosis available," Dr. Brat said.
For the study, Dr. Brat and colleagues performed CT-guided percutaneous thoracic sympathectomy on 50 consecutive men and women with palmar hyperhidrosis. The patients ranged in age from 18 to 37.
In all cases, multi-slice CT fluoroscopy enabled perfect needle guidance. Immediate successful results were observed in 47 patients (94 percent). Three patients underwent a successful second treatment. No significant complications were observed. Sixteen patients experienced minor complications including chest pain and thoracic discomfort, which resolved within a few hours.
The procedure, which can also be used to treat sweaty feet, is less expensive than open or endoscopic surgery and is often covered by insurance.
Dr. Brat cautioned, however, that the treatment is not for everyone. "If you suffer from this condition, it should significantly impair your normal life before you consider this type of treatment," he said. "Although sympathectomy is very effective, it is permanent. You must strike a balance between improvement of your quality of life with this or any other procedure and the potential risks and side effects of treatment."
Dr. Brat advises patients to discuss the risks and benefits with their physicians before undertaking any treatment plan.
Dr. Brat's co-author is Tarik Bouziane, M.D.
# # #
Note: Copies of RSNA 2005 news releases and electronic images will be available online at RSNA.org/press05 beginning Monday, Nov. 28.
RSNA is an association of more than 38,000 radiologists, radiation oncologists, medical physicists and related scientists committed to promoting excellence in radiology through education and by fostering research, with the ultimate goal of improving patient care. The Society is based in Oak Brook, Ill.
Editor's note: The data in these releases may differ from those in the printed abstract and those actually presented at the meeting, as researchers continue to update their data right up until the meeting. To ensure you are using the most up-to-date information, please call the RSNA Newsroom at (312) 949-3233.
| Abstract: |
Images (.JPG format)
 Figure 1. Picture of a doctor preparing CT fluoroscopy guided thoracic sympathectomy. High-res (TIF) version (Right-click and Save As) |
 Figure 2. Example of palmar hyperhidrosis (sweaty hand). High-res (TIF) version (Right-click and Save As) |
 Figure 3. Image of CT-guided neurolysis (percutaneous sympathectomy). |
 Figure 4. Equipment used in CT fluoroscopy. High-res (TIF) version (Right-click and Save As) |
 Figure 5. An illustration of the spine, pinpointing the location where the injection is given in a CT fluoroscopy guided thoracic sympathectomy. High-res (TIF) version (Right-click and Save As) |
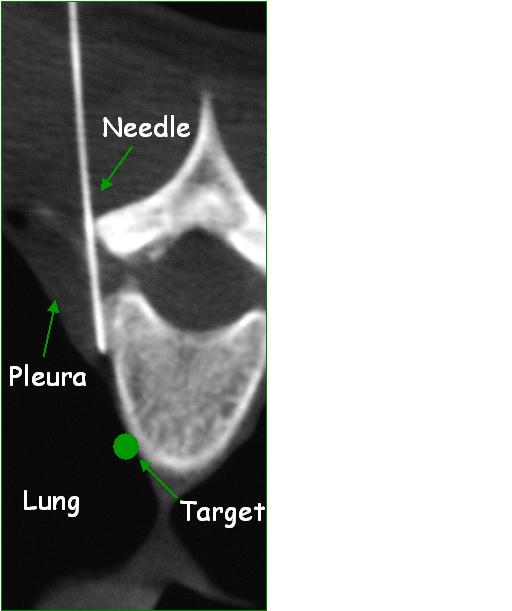 Figure 6. Image showing the location of injection in a CT fluoroscopy guided thoracic sympathectomy. High-res (TIF) version (Right-click and Save As) |
 Figure 7. Image showing the widening of the pleural space in a CT fluoroscopy guided thoracic sympathectomy. High-res (TIF) version (Right-click and Save As) |
 Figure 8. Image showing the contrast and phenol injection in a CT fluoroscopy guided thoracic sympathectomy. High-res (TIF) version (Right-click and Save As) |
 Figure 9. Image pinpointing the location for injection in a CT fluoroscopy guided thoracic sympathectomy. High-res (TIF) version (Right-click and Save As) |
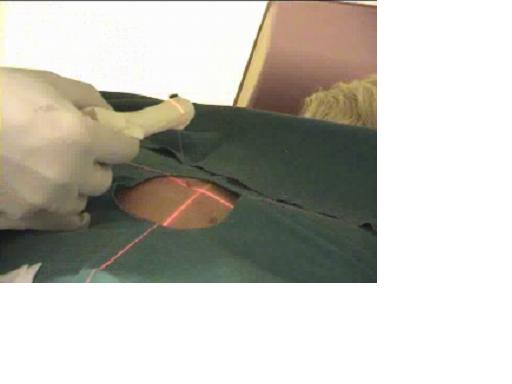 Figure 10. Patient undergoing a CT fluoroscopy guided thoracic sympathectomy. High-res (TIF) version (Right-click and Save As) |
 Figure 11. CT image during a CT fluoroscopy guided thoracic sympathectomy. High-res (TIF) version (Right-click and Save As) |
 Figure 12. Patient prepared to undergo a CT fluoroscopy guided thoracic sympathectomy. |
 Figure 13. Interventional radiology team performing a CT fluoroscopy guided thoracic sympathectomy. |
Figure 14. The technique — showing a needle inserted into the 3rd thoracic vertebra. 1) locating target 2) widening of pleural space 3) contrast and phenal injection. |
 Figure 15. Image of needle inserted into the 3rd thoracic vertebra. |
 PDF
PDF