RSNA Press Release
- Annual mammograms with breast ultrasound or MRI may be sufficient follow up in patients with atypical lobular hyperplasia (ALH) and lobular carcinoma in situ (LCIS) when radiology and pathology findings are benign and concordant.
- ALH and LCIS are abnormal breast lesions associated with an increased risk of cancer.
- The current standard practice is to surgically remove ALH and LCIS lesions; but none of the benign concordant cases in the study was subsequently upgraded to cancer.
Some Women with Abnormal Breast Lesions May Avoid Surgery
Released: July 30, 2013
| Media Contacts: | |
| RSNA Media Relations: | 1-630-590-7762 |
| Linda Brooks 1-630-590-7738 lbrooks@rsna.org |
Maureen Morley 1-630-590-7754 mmorley@rsna.org |
OAK BROOK, Ill. — Surgery is not always necessary for women with a type of breast tissue abnormality associated with a higher risk of cancer, according to a new study published online in the journal Radiology. Researchers said that periodic imaging and clinical exam are effective in these patients when radiology and pathology findings are benign and concordant, or in agreement.
Atypical lobular hyperplasia (ALH) and lobular carcinoma in situ (LCIS) are abnormal breast lesions that occasionally appear as incidental findings in breast biopsies. Women with ALH or LCIS have a four to 10 times higher risk of developing breast cancer, according to Michael A. Cohen, M.D., FACR, professor of radiology at the Emory University School of Medicine in Atlanta. As a result, it is often recommended that ALH and LCIS diagnosed on image-guided core biopsy be removed surgically.
"Because of the possibility of upgrade to cancer, the bulk of the published literature says that the prudent thing to do is excise ALH and LCIS," Dr. Cohen said.
But new research from Dr. Cohen, Kristen Atkins, M.D., and colleagues may alter that thinking.
Dr. Atkins is a pathologist and associate professor at the University of Virginia in Charlottesville, Va. At one time, Drs. Cohen and Atkins were colleagues there and had many discussions about balancing the risk of cancer in ALH and LCIS patients with the costs and potential complications of surgery.
"From a pathology perspective, ALH and LCIS are often very tiny lesions, so we wondered why they were getting excised," Dr. Atkins said. "These surgeries may involve general anesthesia and possible disfigurement."
The researchers studied 10 years of pathology and radiology data to look for a correlation between the number of ALH and LCIS cases that were upgraded to cancer after surgery or follow up and the concordance between the radiologist and pathologist.
The research yielded 50 cases from 49 women aged 40 to 73 years. Radiologist and pathologist findings were concordant in 43 of the 50 cases. None of the benign concordant cases were subsequently upgraded to cancer, strongly suggesting that observation in these patients would have been a viable alternative to surgery. Of the seven discordant cases, two were upgraded to ductal carcinoma in situ, or DCIS, an early-stage, noninvasive form of breast cancer.
Dr. Cohen repeated the study after moving to Emory and found the same results.
"When there's no discordance between the radiologist and pathologist after thorough radiology-pathology correlation, there's no upgrade from ALH or LCIS to cancer in our study," Dr. Cohen said. "These findings show that some women can avoid surgery, and that yearly mammograms along with MRI or ultrasound as second-line screening tools may suffice."
The researchers suggested that their findings will help physicians and patients make informed decisions about ALH and LCIS.
# # #
"Atypical Lobular Hyperplasia and Lobular Carcinoma in Situ at Core Breast Biopsy: Use of Careful Radiologic-Pathologic Correlation to Recommend Excision or Observation." Collaborating with Drs. Cohen and Atkins were Brandi Nicholson, M.D., and Sandra Rao, M.D.
Radiology is edited by Herbert Y. Kressel, M.D., Harvard Medical School, Boston, Mass., and owned and published by the Radiological Society of North America, Inc. (http://radiology.rsna.org/)
RSNA is an association of more than 51,000 radiologists, radiation oncologists, medical physicists and related scientists, promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Ill. (RSNA.org)
For patient-friendly information on MRI and ultrasound, visit RadiologyInfo.org.
Images
 Figure 1: Images in 48-year-old woman with nipple discharge. (a) US scan shows small, irregu¬lar, hypoechoic mass (arrows), for which biopsy was recommended. (b) Low-power photomicrograph (H-E stain; original magnification, 340) of core bi¬opsy specimen reveals normal breast parenchyma with foci of ALH. This was discordant with imaging finding of mass, and surgical excision was recom¬mended. (c) Photomicrograph of surgical specimen (H-E stain; original magnification, 3200) reveals small papilloma, which was fully excised. High-res (TIF) version (Right-click and Save As) |
 Figure 2: (a) Mammogram in 52-year-old woman shows suspicious fine linear branching microcalcifica¬tions (arrow), for which stereotaxic core biopsy was recommended and performed. (b) Radiograph of core specimen obtained at stereotaxic biopsy reveals numerous microcalcifications (circles). (c) Photomicrograph of core biopsy specimen (H-E stain; original magnification, 3 200) reveals only scant benign calcification and foci of ALH (not pictured). The paucity of calcifications identified at histologic examination combined with the benign diagnosis was thought to be discordant, and surgical excision was recommended. (d) Photomicro¬graph of surgical specimen (H-E stain; original magnification, 3400) shows DCIS. High-res (TIF) version (Right-click and Save As) |
 Figure 3: (a) Magnification view of left breast in 62-year-old woman reveals fine pleomorphic micro¬calcifications in segmental distribution (arrows), for which stereotaxic core biopsy was recommended. (b) Radiograph of specimen from stereotaxic biopsy reveals adequate sampling of suspicious microcalcifications (circle). (c) Photomicrograph of specimen (H-E stain; original magnification, 3400) reveals fibrocystic changes with scattered microcalcifications. (d) Although this histologic finding was concordant with imaging features, florid LCIS (H-E stain; original magnification, 3200) was also identified in core specimens and excision was recommended. Final excision showed noncalcified florid LCIS. High-res (TIF) version (Right-click and Save As) |
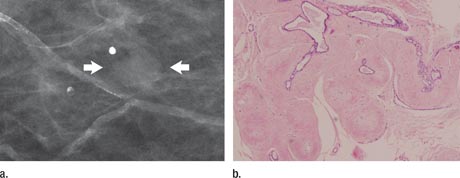 Figure 4: (a) Spot mammogram in 58-year-old woman reveals oval mass with indistinct margins (arrows), for which histologic sampling was recommended. (b) Photomicrograph of core biopsy specimen reveals scle¬rosed fibroadenoma (H-E stain; original magnification, 3200), which is concordant with imaging features. High-res (TIF) version (Right-click and Save As) |
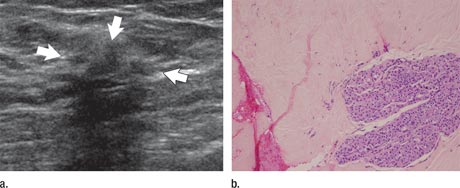 Figure 5 (a) Image in 54-year-old woman with irregular hypoechoic mass (arrows) with posterior acoustic shadowing, for which US-guided core biopsy was recommended. (b) Photomicrograph of core biopsy specimen (H-E stain; original magnification, 340) shows extensive dense sclerosis in all cores (light pink stroma at left and top) and foci of ALH (right). Sclerosis was thought to be concordant with imaging features. Surgical excision revealed only ALH. High-res (TIF) version (Right-click and Save As) |
 PDF
PDF